
Chronic heartburn isn’t just annoying-it can quietly change the lining of your esophagus in ways that put you at risk for something far more serious. For people who’ve had GERD for more than 10 years, especially men over 50, there’s a hidden complication called Barrett’s esophagus. It doesn’t cause new symptoms. You won’t feel it. But it’s the bridge between everyday reflux and esophageal cancer. And most people don’t know they have it until it’s too late.
What Is Barrett’s Esophagus, Really?
Barrett’s esophagus happens when the normal pink, flat lining of your esophagus-designed to handle food, not stomach acid-gets damaged over time. In response, your body tries to repair it by replacing those cells with a different type: columnar cells that look more like the lining of your intestine. This is called intestinal metaplasia. It’s not cancer. But it’s the first step on a path that can lead to it. This change doesn’t happen overnight. It takes at least a decade of frequent acid exposure. Studies show that people with GERD symptoms three or more times a week for over 20 years are 40 times more likely to develop Barrett’s than someone without long-term reflux. And it’s not random: 79% of diagnosed cases are in men. White men over 50 with a history of smoking or obesity are at the highest risk. The scary part? Barrett’s esophagus itself doesn’t cause pain, trouble swallowing, or new symptoms. You still just feel your usual heartburn or regurgitation. That’s why so many people go undiagnosed. The Esophageal Cancer Action Network found that 68% of patients had symptoms for over five years before anyone ever checked their esophagus.How Is It Diagnosed? (It’s Not What You Think)
You can’t diagnose Barrett’s with a blood test, a scan, or even a symptom checklist. The only way is through an upper endoscopy. During the procedure, a doctor threads a thin, flexible camera down your throat. If they see patches of salmon-colored tissue instead of the normal pale lining-especially above the junction where your esophagus meets your stomach-that’s a visual clue. But that’s not enough. They have to take biopsies. Lots of them. The standard is the Seattle protocol: four biopsies every 1 to 2 centimeters along the abnormal area. That means 12 to 24 tissue samples per procedure. Why so many? Because cancer doesn’t spread evenly. It starts in tiny, hidden spots. Missing even one could mean missing the early warning. The pathologist then looks for intestinal metaplasia under the microscope. No metaplasia? You don’t have Barrett’s. Once confirmed, they grade it:- Non-dysplastic Barrett’s (NDBE): No precancerous changes. Most common.
- Indefinite for dysplasia: The cells look weird, but not clearly precancerous. Needs repeat testing.
- Low-grade dysplasia (LGD): Early signs of abnormal cell growth. Risk is low but real.
- High-grade dysplasia (HGD): Cells are severely abnormal. This is the last step before cancer. Up to 19% of HGD cases turn into cancer each year.
Who Should Be Screened? (The Controversy)
This is where things get messy. Not everyone with GERD needs an endoscopy. Screening isn’t free. It’s invasive. And most people with Barrett’s will never get cancer. The American College of Gastroenterology says screen men over 50 who’ve had frequent GERD (weekly or more) for five or more years-and have at least one other risk factor: White race, smoking, obesity, or a family history of esophageal cancer. Women? Generally not recommended, unless they have multiple risk factors. Why? Because the risk is so low in women that the cost and risk of procedures outweigh the benefit. But here’s the problem: many doctors don’t follow this. One Reddit user shared that three different gastroenterologists gave them three different surveillance schedules for the same diagnosis. That inconsistency is real. And it leaves patients confused and anxious. And then there’s the big unanswered question: does screening even save lives? No study has proven that finding Barrett’s early and monitoring it reduces deaths from esophageal cancer. Dr. Stuart Spechler put it bluntly: “We’re doing endoscopies on 95% of people who will never get cancer.”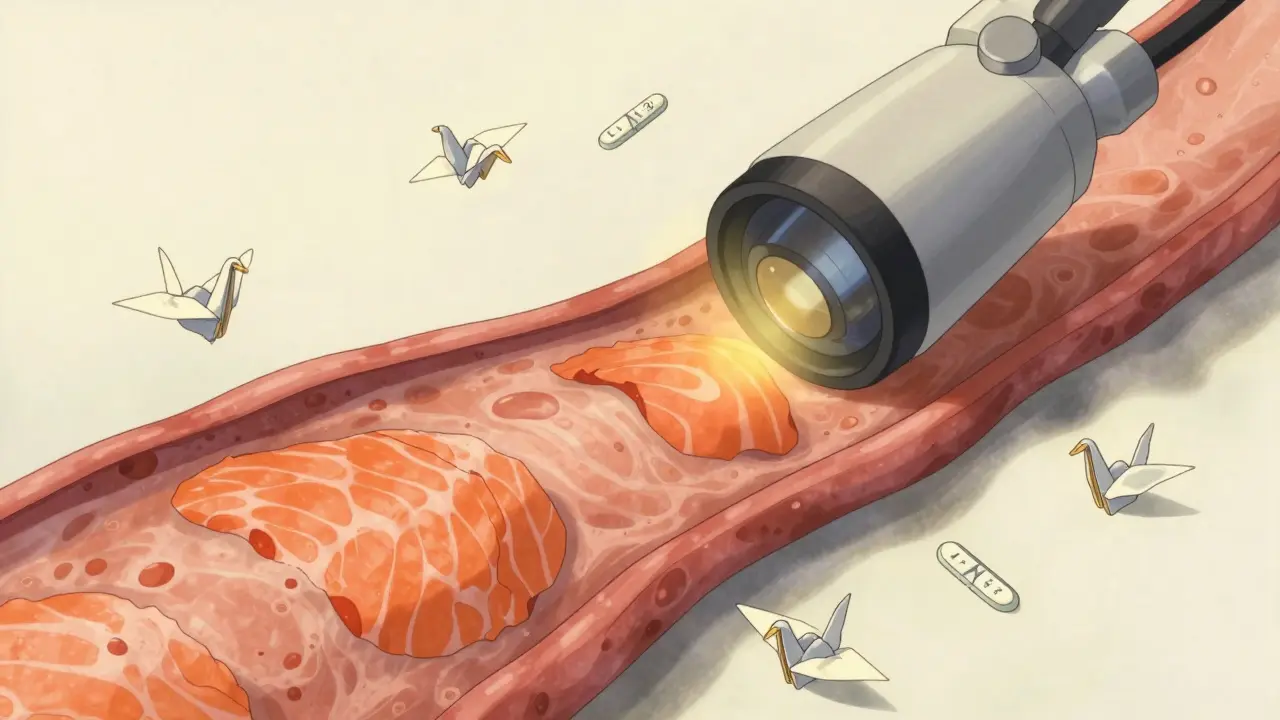
What Happens After Diagnosis?
If you’re diagnosed with non-dysplastic Barrett’s, you’re not being told to panic. You’re told to manage your reflux-and get checked again in 3 to 5 years. That’s it. No drugs, no surgery. Just surveillance. But if you have low-grade dysplasia? The rules changed in 2022. The American Gastroenterological Association now recommends treatment, not just watching. Why? Because a major 5-year study (AIMS-2) showed that 94% of LGD cases could be permanently removed with radiofrequency ablation (RFA). RFA uses heat to burn off the abnormal tissue. It’s quick, outpatient, and works in over 90% of cases. High-grade dysplasia? That’s a red flag. Most doctors skip surveillance entirely and go straight to ablation. Cryotherapy (freezing) is another option. Both have high success rates. After treatment, patients need follow-up endoscopies every 3 to 6 months for a few years to make sure it doesn’t come back.Can You Prevent It? (Lifestyle Matters More Than You Think)
Medication alone won’t cut it. Proton pump inhibitors (PPIs) like omeprazole help with heartburn-but they don’t always stop acid from reaching your esophagus. Studies show only 55-70% of patients get full acid suppression with standard doses. Real protection comes from lifestyle:- Stop eating 3 hours before bed-gravity helps keep acid down.
- Elevate your head 6-8 inches while sleeping. Use blocks under your bed frame, not just extra pillows.
- Avoid trigger foods: fatty meals, chocolate, caffeine, alcohol, spicy food.
- Get your BMI under 25-obesity increases pressure on your stomach and worsens reflux.
- Quit smoking-it relaxes the lower esophageal sphincter and reduces saliva production, which normally neutralizes acid.
The Future: Less Scanning, More Smarts
The future of Barrett’s screening isn’t more endoscopies. It’s better tools. In 2021, Medicare started covering the TissueCypher Barrett’s Esophagus Assay. It’s a non-endoscopic test that analyzes DNA patterns in cells from a swallowable capsule. In a 635-person study, it had a 96% negative predictive value-meaning if it says you’re low risk, you almost certainly are. Researchers in Texas are now testing DNA methylation markers that could predict who’s likely to progress to cancer. If it works, we could cut unnecessary endoscopies by 40%. That’s huge-both for patients and the healthcare system. Right now, the U.S. spends $1.2 billion a year on Barrett’s screening and surveillance.What Should You Do?
If you’ve had daily heartburn for over 10 years-especially if you’re a man over 50, White, overweight, or a smoker-talk to your doctor. Don’t wait for symptoms to get worse. Ask: “Should I be screened for Barrett’s esophagus?” If you’ve already been diagnosed, don’t ignore follow-ups. Even non-dysplastic Barrett’s needs monitoring. And if you’re on PPIs, ask if your dose is enough. Some people need twice-daily dosing to truly suppress acid. Barrett’s esophagus isn’t a death sentence. Most people live normal lives with it. But it’s a silent threat. And the only way to beat it is to know you have it-and act before it turns into something worse.Can Barrett’s esophagus go away on its own?
No. Once the esophagus lining changes to intestinal metaplasia, it doesn’t revert back on its own. But it can be removed. Radiofrequency ablation and cryotherapy can eliminate the abnormal tissue in over 90% of cases. After treatment, the normal lining can regrow-especially if acid exposure is fully controlled.
Do proton pump inhibitors (PPIs) prevent Barrett’s from turning into cancer?
Not necessarily. While PPIs help with heartburn, studies show they don’t always stop acid from reaching the esophagus. Even if symptoms disappear, reflux can still be happening. Complete acid suppression-confirmed with pH monitoring-is what’s needed to protect the esophagus. That’s why lifestyle changes are just as important as medication.
Is Barrett’s esophagus the same as esophageal cancer?
No. Barrett’s esophagus is a precancerous condition. It’s a change in the cell type lining the esophagus. Only about 5% of people with Barrett’s will develop esophageal adenocarcinoma over their lifetime. But because that cancer is aggressive and often found late, the survival rate is low-less than 20% at five years. That’s why early detection matters.
Can women get Barrett’s esophagus?
Yes, but it’s much less common. Men are diagnosed with Barrett’s three times more often than women. Screening is generally not recommended for women unless they have multiple risk factors: long-term GERD, obesity, smoking, and a family history of esophageal cancer. The risk in women without these factors is so low that screening isn’t considered cost-effective.
What’s the difference between low-grade and high-grade dysplasia?
Low-grade dysplasia (LGD) means some cells look abnormal under the microscope, but they’re still mostly organized and not deeply changed. It’s like a warning sign. High-grade dysplasia (HGD) means the cells are severely disorganized, look very different from normal, and are much closer to becoming cancer. HGD carries a 6-19% annual risk of turning into cancer. Most doctors treat HGD immediately with ablation, not surveillance.



9 Comments
Ethan Zeeb- 3 March 2026
Barrett’s isn’t some myth. I had it. No symptoms beyond my usual heartburn. Got screened because my dad died of esophageal cancer. Endoscopy found non-dysplastic. They told me to watch my diet and come back in 5 years. I quit smoking, lost 40 lbs, and stopped eating after 7 p.m. No more meds. Just discipline. If you’re over 50 and have had GERD for a decade, get checked. Don’t wait until you’re coughing up blood.
Darren Torpey- 3 March 2026
Bro, this is the kind of post that makes you wanna hug a gastroenterologist. 😭
Barrett’s is like your body’s silent protest against your 3 a.m. burrito habit. It’s not screaming-it’s whispering, ‘Hey, maybe stop turning your esophagus into a pizza delivery chute?’
And RFA? That’s basically giving your esophagus a spa day with lasers. 90% success rate? I’ll take that over a lifetime of Prilosec.
Mariah Carle- 4 March 2026
It’s funny how we treat our bodies like rental cars-drive ‘em hard, ignore the warning lights, then act shocked when the engine blows.
Barrett’s is the universe’s way of saying: ‘You didn’t listen to your body because you were too busy scrolling memes while eating a whole pizza alone.’
But here’s the twist-it’s not about guilt. It’s about grace. You can still change the story.
❤️
Justin Rodriguez- 5 March 2026
Just want to clarify something from the article: the Seattle protocol isn’t arbitrary. Taking 12–24 biopsies isn’t overkill-it’s because dysplasia is patchy. Missing even one 2mm area can mean missing early cancer.
Also, PPIs don’t fix the underlying motility issue. They just reduce acid. Lifestyle changes are non-negotiable. Elevating the bed? It’s not a gimmick. Gravity still works.
Siri Elena- 7 March 2026
Oh honey. You mean to tell me after 10 years of eating tacos while lying on the couch, your body decided to upgrade your esophagus to a ‘premium intestinal suite’? How poetic.
And now you’re surprised? Sweetie, if your reflux has its own Netflix account, you’ve been ignoring the red flags since 2014.
But hey-your doctor’s not wrong. Just… you know… maybe stop treating your throat like a trash compactor? 💅
Jane Ryan Ryder- 8 March 2026
Screening? For who? White men? So now it’s a race thing? Great. Just what we needed. Another medical excuse to ignore women.
My mom had GERD for 20 years. Never got screened. Died of cancer at 62. Guess she wasn’t ‘high risk’ enough.
Stop pretending this is science. It’s bias with a stethoscope.
Callum Duffy-10 March 2026
The data on screening is indeed complex. While the ACG guidelines are evidence-based, real-world implementation remains inconsistent. I’ve reviewed multiple studies from the UK and Canada-there’s no mortality benefit demonstrated in population-level screening. The cost-benefit analysis is tenuous.
However, targeted screening in high-risk cohorts-particularly those with multiple risk factors-remains clinically prudent. The future lies in biomarkers, not endoscopies.
Chris Beckman-11 March 2026
Bro I had this and I’m 32 and I’m not even white. I’m mexican. I just had bad reflux since I was 22. Got an endo and they said I had LGD. They did RFA and it’s gone. Now I don’t even take ppi. Just sleep on a wedge and no pizza after 8.
Point is: it’s not just old white dudes. Anybody with long term reflux should get checked. I’m not even 50. 😅
Richard Elric5111-12 March 2026
It is imperative to recognize that the pathophysiological transition from chronic gastroesophageal reflux to intestinal metaplasia constitutes a paradigmatic example of adaptive cellular reprogramming under persistent inflammatory stress. The notion that this transformation is merely a ‘precancerous’ condition is reductive; it is, in fact, a systemic biomarker of prolonged physiological neglect.
Therefore, screening protocols must be reconceptualized not as diagnostic tools, but as ethical imperatives within a biopsychosocial framework of preventive medicine.