
Pancreatic Duct Blockage Symptom Checker
Severe Abdominal Pain
Persistent, intense pain in the upper abdomen that radiates to the back lasting more than a few hours.
Jaundice
Yellowing of skin or eyes along with dark urine, indicating bile flow issues.
Nausea/Vomiting
Persistent nausea or vomiting that doesn't improve with over-the-counter remedies.
Fever
Fever over 38°C (100.4°F) or chills, suggesting possible infection.
Weight Loss
Unexplained weight loss or appetite loss over weeks.
Abdominal Swelling
Sudden swelling in the abdomen or feeling of fullness.
Key Takeaways
- Pancreatic duct blockage can cause sudden, severe abdominal pain and jaundice.
- Common culprits are gallstones, chronic pancreatitis, and tumors.
- Seek medical help if pain lasts more than a few hours, you develop fever, or notice yellowing of skin/eyes.
- Diagnosis relies on blood tests and imaging such as CT, MRI, or ERCP.
- Treatment ranges from endoscopic stenting to surgery, depending on cause.
pancreatic duct blockage is a condition that most people only hear about when they’re in the middle of a painful episode. Understanding what it is, why it happens, and when to call a doctor can turn a scary situation into a manageable one.
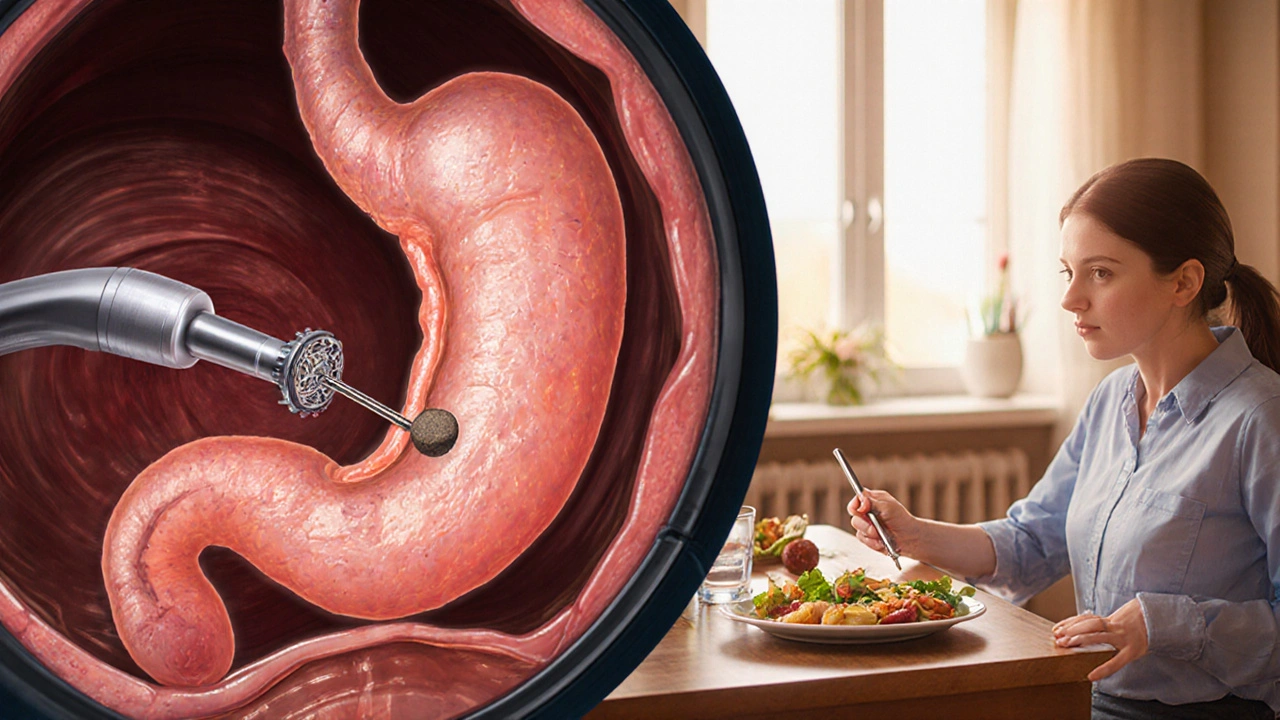
What Is Pancreatic Duct Blockage?
When the narrow tube that carries digestive enzymes from the pancreas a gland located behind the stomach that produces insulin and digestive enzymes into the small intestine becomes obstructed, the enzymes back up. This backup can inflame the pancreas, damage nearby tissue, and trigger a cascade of symptoms that range from mild discomfort to life‑threatening organ failure.
Common Causes
Several conditions can clog the duct:
- Gallstones hard particles formed from cholesterol or bilirubin that can migrate into the pancreatic duct. They are the leading cause of sudden blockage.
- Chronic pancreatitis long‑term inflammation that produces scar tissue narrowing the duct. Alcohol abuse and high‑fat diets are frequent risk factors.
- Pancreatic cancer malignant growths that can press on or grow within the duct. Though rarer, it demands urgent attention.
- Benign tumors such as intrapancreatic cysts fluid‑filled sacs that can expand and block flow.
- Injuries or post‑surgical scar tissue that inadvertently narrow the channel.

Typical Symptoms and Red Flags
Because the pancreas sits deep in the abdomen, pain can be misleading. Look for this pattern:
- Severe, steady upper‑abdominal pain that radiates toward the back and lasts longer than a couple of hours.
- Nausea or vomiting that doesn’t improve with over‑the‑counter remedies.
- Yellowing of the skin or eyes (jaundice a sign that bile flow is compromised), especially if accompanied by dark urine.
- Unexplained weight loss or appetite loss over weeks.
- Fever, rapid heartbeat, or a sudden drop in blood pressure - these indicate possible infection or sepsis.
If any of these appear together, treat them as an emergency.
When to Call a Doctor
Knowing the line between "watchful waiting" and "need immediate care" saves lives. Call your GP or head straight to the emergency department when:
- Pain persists for more than 4hours or worsens despite rest.
- You develop fever>38°C (100.4°F) or feel chills.
- Yellowing of skin/eyes appears.
- Vomiting is frequent (more than 3 times in an hour) or you cannot keep fluids down.
- You notice sudden swelling in the abdomen or a feeling of fullness.
Even if the pain subsides, get evaluated within 24hours because the underlying blockage may still be present and could cause recurrence.
How Doctors Diagnose the Problem
Diagnosis is a step‑by‑step process that blends lab work with imaging:
- Blood tests: Levels of amylase an enzyme that spikes when the pancreas is inflamed and lipase another pancreatic enzyme that remains elevated longer than amylase are measured. Elevated bilirubin suggests bile‑duct involvement.
- Ultrasound: A quick, bedside tool that can detect gallstones and dilated ducts.
- CT scan (computed tomography) or MRI (magnetic resonance imaging): Provide detailed cross‑sectional pictures, revealing tumors, cysts, or severe inflammation.
- Endoscopic Retrograde Cholangiopancreatography (ERCP): A thin endoscope is passed down the throat to inject contrast into the pancreatic duct, visualizing the exact blockage point. It also allows for therapeutic interventions like stent placement.
- Endoscopic ultrasound (EUS): Combines endoscopy with high‑frequency sound waves to image small lesions that CT may miss.
The specialist you’ll see is usually a gastroenterologist a doctor who focuses on the digestive system and performs ERCP. In complex cases, a hepatobiliary surgeon a surgeon specializing in liver, gallbladder, and pancreas operations may be consulted.
Treatment Options Overview
Treatment is tailored to the underlying cause:
- Endoscopic stone removal: During ERCP, tiny baskets or lithotripsy devices break up gallstones, clearing the duct.
- Stent placement: A small tube holds the duct open while the underlying inflammation heals.
- Medication: Pancreatic enzyme supplements reduce the pancreas’s workload; antibiotics are given if infection is present. \n
- Surgical options: For tumors or persistent strictures, procedures like the Whipple operation (pancreaticoduodenectomy) or distal pancreatectomy may be necessary.
- Lifestyle modifications: Low‑fat diets, complete alcohol abstinence, and maintaining a healthy weight lower recurrence risk.
Recovery timelines differ. Endoscopic relief often yields rapid symptom improvement within days, whereas surgery may require weeks of recuperation.
Living With or After a Blockage
Even after the duct is cleared, you’ll want to keep future episodes at bay:
- Follow a low‑fat, high‑protein meal plan. Aim for <30g of fat per day.
- Stay hydrated; adequate fluids help thin pancreatic secretions.
- Avoid alcohol completely-even occasional drinks can reignite inflammation.
- Schedule regular follow‑up imaging (usually ultrasound or MRI) every 6-12months if you had a tumor or chronic pancreatitis.
- Keep a symptom diary. Noting pain patterns, food intake, and medication response helps your doctor adjust treatment.
Frequently Asked Questions
Can a pancreatic duct blockage resolve on its own?
Rarely. Small gallstones may pass, but most blockages need medical or endoscopic intervention to prevent complications.
Is the pain always in the upper abdomen?
Usually, but the pain can radiate to the back, chest, or even the left shoulder. The pattern varies with the blockage’s location.
What’s the difference between ERCP and EUS?
ERCP injects contrast into the ducts to visualize and treat blockages; EUS uses an ultrasound probe on the same endoscope to create detailed images, mainly for diagnosis.
Will I need lifelong enzyme supplements?
If permanent duct damage occurs, supplements may be required indefinitely. Your doctor will test enzyme levels before deciding.
Are there any warning signs that a blockage is becoming an emergency?
Sudden high fever, rapid heartbeat, confusion, or a drop in blood pressure are red flags. Call emergency services immediately.
Comparison of Common Causes of Pancreatic Duct Blockage
| Cause | Typical Symptom | Preferred Test |
|---|---|---|
| Gallstones | Sudden upper‑abdominal pain, radiating to back | Ultrasound → ERCP if stone seen |
| Chronic pancreatitis | Recurrent pain, weight loss, oily stools | CT scan with contrast |
| Pancreatic cancer | Jaundice, new‑onset diabetes, persistent pain | MRI or Endoscopic ultrasound |
| Intrapancreatic cyst | Vague discomfort, occasional nausea | EUS for detailed imaging |
Remember, early recognition and prompt medical evaluation are the best defenses against serious complications. If you suspect a blockage, don’t wait-reach out to a healthcare professional right away.


19 Comments
kevin muhekyi- 9 October 2025
I've been reading up on pancreatic duct issues, and it's crazy how something so small can cause such big pain. The article nails the key red flags like persistent upper‑abdominal pain and jaundice. If you notice any of those, don't wait – get to a doctor ASAP. Staying aware can save you from a nasty surprise.
Teknolgy .com-13 October 2025
Wow, another medical checklist – feels like a pop‑up ad for panic. 🤔 But hey, at least it reminds you to watch for fever and swelling.
Caroline Johnson-18 October 2025
Seriously?? This write‑up throws a *lot* of warnings at you, and for good reason!!! The pancreas is tucked away, so pain can be deceiving, and missing the signs can be disastrous!!! You *must* heed the portion about jaundice, fever, and pain lasting more than four hours – they are not optional symptoms!!!
Megan Lallier-Barron-22 October 2025
Interesting take, but I think people sometimes overreact to mild nausea. 😐 The body can handle a little upset without a trip to the ER. Just keep an eye on it and stay hydrated.
Kelly Larivee-26 October 2025
The main thing is to notice the pain and yellowing. If it shows up, call your doctor fast. Simple as that.
Emma Rauschkolb-30 October 2025
🤒 The clinical picture you described – elevated amylase, bilirubin spikes, and systemic inflammatory response – screams acute pancreatitis due to ductal obstruction. Immediate imaging (CT or MRCP) is non‑negotiable. Otherwise, you risk progressing to sepsis. Stay vigilant!
Kaushik Kumar- 3 November 2025
Hey everyone!!! Remember, early detection is the hero here!!! If you spot severe pain, fever, or jaundice, don’t wait – head to the ER or call your GP right away!!! The sooner you get proper labs and imaging, the better your outcomes!!! Keep looking after yourselves, friends!!!
Mara Mara- 7 November 2025
It's crucial to understand that pancreatic duct blockage can stem from gallstones, strictures, or neoplasms. Prompt diagnosis via ultrasound or CT is essential. Timely intervention, whether endoscopic or surgical, improves prognosis. Stay informed and seek care without delay.
Jennifer Ferrara-12 November 2025
In sumary, the authors have provided a comprehensive overview of the etiologies and clinical manifestations associated with pancreatic duct obstruction. The inclusion of both diagnostic algorithms and therapeutic options enhances the utility of the piece. However, a more detailed discussion on post‑procedure follow‑up could be beneficial. Overall, it serves as a valuable resource for both clinicians and patients alike.
Terry Moreland-16 November 2025
That sounds really scary, and it's understandable to feel overwhelmed. The key is to act quickly if you notice the red‑flag symptoms listed. Getting checked early can prevent complications. I'm wishing anyone dealing with this a smooth recovery.
Abdul Adeeb-20 November 2025
It is imperative that patients exhibiting persistent epigastric pain, jaundice, or fever seek immediate medical evaluation. Delays in diagnosis may precipitate irreversible pancreatic damage. Appropriate laboratory assays and imaging modalities should be employed without hesitation. Early therapeutic intervention remains the cornerstone of favorable outcomes.
Abhishek Vernekar-24 November 2025
Yo, thanks for the breakdown! 😊 If you get that kind of pain, don't mess around – go to the hospital. The docs will sort out the blockage fast.
Val Vaden-28 November 2025
This article is way overhyped.
lalitha vadlamani- 2 December 2025
Behold, the silent assassin that lurks within our bodies, whittling away at health with insidious stealth! One cannot simply dismiss the grave peril of a blocked pancreatic duct as trivial. The very notion that such a condition can precipitate organ failure demands reverence. Let all who read this be warned, lest hubris lead them to ignore the warning signs! May prudence guide your actions.
kirk lapan- 7 December 2025
Honestly, anyone who says “just wait it out” clearly never saw a CT of a blocked duct. The pancreas isn’t some “maybe” organ – it’s a powerhouse, and when its flow is blocked, you’re looking at potential necrosis. I’ve read dozens of case studies where delays lead to sepsis, and that’s not some myth. So, if you’ve got those symptoms, get to an ER pronto, no debate.
Tara Phillips-11 December 2025
The clinical significance of pancreatic duct obstruction cannot be overstated, as it represents a nexus of potential acute and chronic pathologies.
The prompt recognition of hallmark symptoms such as persistent upper abdominal pain, unexplained jaundice, and fever is the first decisive step toward favorable outcomes.
Diagnostic rigor demands a sequential approach, beginning with serum amylase and lipase measurements to assess enzymatic elevation.
Subsequent imaging, preferably a contrast‑enhanced CT scan, offers detailed visualization of ductal dilatation and possible obstructive lesions.
When CT is inconclusive, magnetic resonance cholangiopancreatography (MRCP) provides superior soft‑tissue contrast without ionizing radiation.
Endoscopic retrograde cholangiopancreatography (ERCP) not only delineates the blockage but also permits therapeutic interventions such as stent placement.
Therapeutic strategies must be tailored to the underlying etiology, with gallstone extraction, stricture dilation, or oncologic resection considered as appropriate.
Pharmacologic support, including pancreatic enzyme supplementation and broad‑spectrum antibiotics when infection is suspected, complements procedural management.
Nutritional optimization, emphasizing low‑fat, high‑protein intake, mitigates the risk of recurrent episodes and supports pancreatic healing.
Patients should be counseled on the avoidance of alcohol and tobacco, both of which exacerbate pancreatic inflammation.
Long‑term follow‑up through periodic imaging and laboratory assessment is essential to monitor for restenosis or malignant transformation.
Multidisciplinary care, involving gastroenterologists, surgeons, radiologists, and nutritionists, ensures comprehensive management.
Education of patients and their families about warning signs empowers them to seek care before complications ensue.
In summary, an integrated approach that couples early detection, precise diagnostics, and targeted therapy yields the best prognosis.
Thus, vigilance and timely action remain the cornerstones of effective treatment for pancreatic duct blockage.
Derrick Blount-15 December 2025
One might argue that the human body is a delicate tapestry, woven with arteries, ducts, and secretions; yet when a single thread like the pancreatic duct is snagged, the entire pattern unravels. This observation underscores the importance of early detection, a principle echoed across countless clinical narratives. Therefore, vigilance is not merely advisable-it is ethically imperative. Let us, as a collective, champion proactive health monitoring.
Anna Graf-19 December 2025
Watch those symptoms closely.
Jarrod Benson-23 December 2025
Man, that was a solid run‑down, Tara! I totally agree-catching the signs early saves a ton of trouble down the line. Keep spreading the knowledge, and folks, don’t wait till you’re in the ER to act.